There is a growing body of research to support the use of Cognitive Behavioral Therapy as part of an integrative approach to migrainetreatment. CBT won’t replace headache specialists, preventive therapies, or acute medical interventions. It can help with one of our biggest triggers though.
Stress
Many migraineurs cite stress as their #1 trigger. The theory is that CBT can help patients increase their tolerance level and reduce the number of attacks triggered by stress. One of the strategies used in CBT is to challenge and change the way a patient thinks aboutmigraine as it relates to their lives.
Negative feedback loop
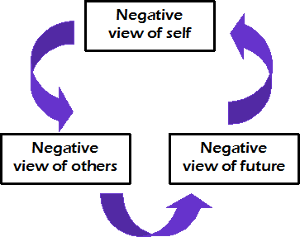
It starts with the idea that negative thinking patterns about yourself, others, and your future create a self-sustaining feedback loop that can affect your whole outlook on life. Breaking the cycle of negative thinking requires us to change the way we think about ourselves, our relationship to others, and our outlook on the future. The way with think about migraine can become an ever-increasingly negative pattern. We can break that cycle by catching our thinking mistakesand correcting those errors.

It works for me
I am just as guilty as everyone else of getting caught in this negative thought/belief pattern many times. Because I have comorbid depression, I am more susceptible to giving in to this kind of thinking. I have to work harder to make sure my thoughts are consistent with reality. The use of CBT strategies has helped to keep my depressive symptoms in remission. It also helps me to manage stress better so I am less vulnerable to those nasty let-down migraine attacks.
Thinking errors
#1 – Drawing a broad conclusion based on irrelevant or insufficient evidence.
Example: “This is my last option.”
I made this mistake when I pursued a “cure” by trying to qualify fortrigger site release surgery. I believed it was the only availabletreatment in my city. That wasn’t true. I just wasn’t willing to look hard enough. I was in a hurry to find a solution, so I didn’t do all of my homework. If you’d asked me back then, I would have denied it. However, the fact that I found several other options after I’d been turned down for surgery proves that my thinking was faulty.
#2 – Focusing on a single aspect of a situation and ignoring others
Example: “There’s nothing left to try.”
I made this mistake when I found out I didn’t qualify for trigger site release surgery. Because I focused on surgery as my only option, I was devastated when it didn’t work out. It took me weeks to finally recognize the truth. There were other treatments to try and otherdoctors to see. I just had to look harder. I tried two more doctors and 6 more treatments before finally finding my current doctors and effective treatments.
#3 – Exaggerating the importance of undesirable events
Example: “I can’t take one more day.”
This was my thinking after getting turned down for surgery. That thought nearly drove me to take my own life. It seems silly now, but in the middle of those thoughts I couldn’t break free. I was so tired of hurting all the time. At least for me, surgery was a passive way to have somebody else fix my problem. In truth, I could tolerate many more days. I know this now because I have done it. If someone had told me in the middle of that darkness that I would face at least 2 more years before getting results, I probably would have given up. Thankfully I was able to focus on getting through one day at a time. Gradually I was able to cope for several days, looking forward to that next appointment. Before long, I had abandoned my lethal plans. My outlook changed because I was able to change how I saw myself and my doctors.
#4 – Underplaying the significance of an event
Example: “I’m fine.”
Don’t we all say this? We minimized our own pain because we rationalize that 1) no one cares to know the truth, 2) we’ve been worse off, or 3) we really don’t want the negative attention. By doing this, we downplay the severity of our symptoms. What’s worse, we do it with our doctors! I’m not suggesting we exaggerate our experiences. Let’s just be honest – any single migraine attack sucks. We’re not fine. We may be fine in a few hours or days, but in the middle of an attack, we are anything but fine.
#5 – Drawing a broad negative conclusion based on a single insignificant event
Example: “Doctors are no help.”
We make a sweeping generalization about all doctors without having tried to work with more than a handful. To be honest, there are some doctors who aren’t any help to us. But that doesn’t mean none of them can help. I know this because I work with two amazing doctors who have helped me a great deal. Neither one of them are UCNS certified and you won’t find them listed on any registry. I’ve also met some very caring, helpful headache doctors. They’re not my doctors, but I know they are helpful because my friends are helped by them. Many of us make this mistake when our doctor tells us there are no more options to try. Just because one, or two, or ten doctors run out of options doesn’t mean there aren’t doctors with new ideas who can help us.
#6 – Attributing the negative feelings of others to yourself
Example: “My husband blames me for always being in pain.”
I made this thinking error many times. When I finally started inviting my husband to talk about the effects of migraine on his life, I learned something very different. Sure, he was frustrated, angry, resentful, and exhausted. He didn’t blame me. He blamed migraine. There’s a big distinction. I get frustrated, angry, resentful, and exhausted because of migraine, too. Once we both realized we were angry about the same thing, we were able to view each other as partners again. The antidote to this mistake is to talk with the person. Ask questions. Listen carefully. Keep an open mind. It may feel as though you are the target of someone’s negative emotions, but that doesn’t make it true. Even if someone does blame you for your migraine, that isn’t necessarily true. They may be guilty of thinking mistakes too.
Interested in learning more about Cognitive Behavioral Therapy and how it can help you with migraine? More articles are in the works that will address different CBT strategies you can use at home.
If you are not familiar with CBT, it might also be a good idea to find a therapist who specializes in CBT for chronic pain. A good starting place is the “Find a Healthcare Provider” tool at ACHEnet.org. When you search, make sure to select the Psychiatry/Psychology/Behavioral Medicine option under Specialty. The providers listed are those who have a good understanding of the impact that migraine has on a patient’s life. They will likely be more sympathetic to your challenges than the average CBT therapist.
