Galleries
Saturday Afternoon Thoughts
I’m stuck. Drowning. No one around to help. Anxiety. Panic attack. Fear of the unknown. Terrified of the future. Out of control. Scared of everything. Worried about everything. My brain is going hundreds of miles an hour. My feet aren’t moving. I can’t go forward. I can’t go back. I don’t want to stay here, stuck. I have to make a move. Trust myself to make the right decision. Pull myself out of this mindset. Take control of the fear and panic. Fight the depression and anxiety. Control what I can. Deal with what I can’t. Take a deep breath. One minute at a time if that’s what it takes. Slow my thought process. Concentrate on one thing at a time. Get through the next five minutes. Then the next five. I can do this. I’ve done it before. Deep breaths. Calming thoughts. Inhale, exhale. Put one foot in front of the other. Take my time. Find one thing to be positive about and hold on to that one thing tightly. Stop overwhelming myself with doubt. Know that I am not alone. And that I’ll be okay. Just not today. #AlwaysKeepFighting
Understanding Migraine Disease and Migraineurs
By Teri Robert patient
patient educator/advocate, author Chair, American Headache and Migraine Association
If you’re reading this, someone close to you is a Migraineur, someone diagnosed with migraine, a genetic neurological disease. Migraine is one of the most misunderstood, underdiagnosed, and undertreated of all diseases. Unless you’ve experienced the pain and other debilitating symptoms of migraine yourself, it can be difficult to understand until you learn more about it. It is not an exaggeration to say that some people have taken their lives to escape the pain. In addition to sometimes extreme head pain, migraine can be accompanied by other symptoms including nausea, vomiting, dizziness, extreme sensitivity to light and sound, temporary loss of vision, inability to concentrate, difficulty in speaking/finding the right words, depression, panic attacks, and far more.
The slightest movement can cause such pain that migraineurs have described it as “an ice pick in my eye,” “my head breaking into pieces,” and “my brain is exploding.” To put it plainly, migraine can be be absolutely devastating.
Here are some basics about Migraine Disease that you should know:
Based on the most recent U.S. census statistics, Migraine disease affects more than 37 million people in the United States alone.
Migraines are NOT headaches. Migraine is a genetic neurological disease, similar in some ways to epilepsy. The head pain of a migraine attack is only one possible symptom of an episode of migraine disease, just as a seizure is only one symptom of an episode of epilepsy.
Migraine disease is NOT a psychological disorder. The disease and all its symptoms are neurological in origin and very, very real. Migraineurs are not neurotic, lazy, “high-strung,”overly emotional, or faking. They are in very real pain and physical distress.
Not all doctors have the experience and knowledge to properly treat migraine. Finding a doctor to properly treat migraine is one of the most important, and sometimes most difficult, steps in treatment.
There is NO CURE for migraine. Most migraineurs, with the help of a qualified doctor, can find preventive regimens that will prevent many, but not all, Migraine attacks.
Migraine abortive medications such as Imitrex, Zomig, Maxalt, Amerge, Axert, DHE, and Migranal, do not work for all migraineurs. It is sometimes very difficult to find medications that will relieve the pain and other symptoms of a migraine attack.
Migraine attacks can be dangerous. Just having migraine disease increases the risk of stroke, heart attack, and other cardio- and cerebrovascular events and diseases.
A migraine attack can, in rare cases, actually be fatal. An otherwise healthy 21-year-old member of our community died of a migrainous stroke in November, 2001.
Migraine disease can be disabling for some migraineurs to the extent that they qualify fordisability income or qualify for accommodation under Americans with Disability Act. There are many whose disease is so severe that doctors are unable to control the attacks, and the migraineur is unable to work or participate in “normal” daily activities. When a migraine attack strikes, most migraineurs desperately need a dark, quiet place to lie down.
Migraine attacks can be triggered by many things:
o Perfumes and fragrances from other sources are a very common Migraine trigger.
If you live or work with a Migraineur, please refrain from wearing fragrances around them.
o Bright and/or flickering lights, especially fluorescent lighting — some migraineurs need to wear sunglasses, even inside.
o Many foods can be triggers, especially foods prepared with MSG.
o Loud noises and crowded places can also be triggers.
o Changes in weather are triggers for many migraineurs.
o Cigarette smoke, exhaust fumes can be strong triggers.
o Each migraineur’s triggers vary. There are many other potential triggers. This list is just a beginning.
o Stress: There is still some controversy about whether stress itself is a Migraine
trigger or an exacerbating factor that makes o Perfumes and fragrances from other sources are a very common Migraine trigger.
If you live or work with a Migraineur, please refrain from wearing fragrances around
them.
o Bright and/or flickering lights, especially fluorescent lighting — some migraineurs
need to wear sunglasses, even inside.
o Many foods can be triggers, especially foods prepared with MSG.
o Loud noises and crowded places can also be triggers.
o Changes in weather are triggers for many migraineurs.
o Cigarette smoke, exhaust fumes can be strong triggers.
o Each migraineur’s triggers vary. There are many other potential triggers. This list is just a beginning.
o Stress: There is still some controversy about whether stress itself is a Migraine trigger or an exacerbating factor that makes migraineurs more susceptible to their other triggers.
The Migraineur(s) in your life need your help and understanding. They need you to realize that they cannot help being ill, they are not “having headaches for attention,” and they are sometimes unable to care for themselves. If they need medical attention, they need someone to take them and be with them. As well as being extremely painful physically, migraine can be devastating emotionally and to relationships and careers. Since the disease is so misunderstood, migraineurs often feel alone, isolated, and desolate. They also often feel guilty because they are not able to “be there” for their family and friends as much as they want to be and because they may have to miss days of work. The migraineur(s) you know need not only your help with getting their medicines and any medical care they may need; they need your moral support every bit as badly. A good, solid support system is as important to Migraineurs as their health care teams. YOU are very important to them. That’s why it’s important that you understand Migraine.
If you have any questions or need more information, please email me at teri@terirobert.com.
Sincerely
Teri Robert
©Teri Robert, 2001 – Present
Last updated February 3, 2015. 
http://www.HelpForHeadaches.com • http://www.HealthCentral.com/migraine • http://www.MigraineAdvocacy.org
September Sunday
 Well, it’s Labor Day weekend. End of another summer. No beach trips. No cookouts. No concerts. No movies. No outings that I would probably have had to cancel anyway. Not worth the stress of “this could happen”, “what if?!”, or disappointment. Better to stay home. My safe haven. My bubble. The only place I can control. Dark, quiet, scent-free. I miss the movies, but the lights and noise level would chase me home. The concerts were so much fun, but too loud and so many people wearing so many scents. The beach was my favorite. But the sun, which I once loved, is now my enemy. All of the simple pleasures in my life have turned into stressors. Reasons for panic and anxiety. Unneeded worry. All chasing me back to my house. My cage. My jail. Don’t get me wrong, it’s comfortable, cozy, relaxing, and safe. But once in awhile, even inmates get yard time. I’m lonely. My only contact with the “outside world” is my computer. I’m blessed to have such good, loyal, understanding, empathetic online friends. My “real life” friends have all abandoned me. No reasons given. Embarrassed?! Tired of my constant cancelling?! Unable to handle my pain?! Whatever the reason, they’re gone. My best friend, secret keeper, confidante, “let’s grow old together” friend, gone. Without a word. It’s easier online. They can’t see my tears, my fears, my hurt, my pain. We talk about it, but it’s not the same as face to face. I see a psychologist. She helps me put things into perspective. My losses, my grief, my fears, my hopes. And yes, I do still have hope. I have to hold on to something. Have a purpose. A reason to wake up and face each new day. Praying for relief, a cure, strength, positive thoughts. Helping others going through similar circumstances. It helps me to help them. To feel like I make a difference to someone in physical and emotional pain. To someone depressed, anxious, panic-filled, like me. We’re strong for each other. Hold each other up. Always reachable. Through new meds, side effects, tests, diagnoses. Bringing laughter to a dark time. But always praying for better days ahead. We must. There is no alternative. Not for me. #AlwaysKeepFighting
Well, it’s Labor Day weekend. End of another summer. No beach trips. No cookouts. No concerts. No movies. No outings that I would probably have had to cancel anyway. Not worth the stress of “this could happen”, “what if?!”, or disappointment. Better to stay home. My safe haven. My bubble. The only place I can control. Dark, quiet, scent-free. I miss the movies, but the lights and noise level would chase me home. The concerts were so much fun, but too loud and so many people wearing so many scents. The beach was my favorite. But the sun, which I once loved, is now my enemy. All of the simple pleasures in my life have turned into stressors. Reasons for panic and anxiety. Unneeded worry. All chasing me back to my house. My cage. My jail. Don’t get me wrong, it’s comfortable, cozy, relaxing, and safe. But once in awhile, even inmates get yard time. I’m lonely. My only contact with the “outside world” is my computer. I’m blessed to have such good, loyal, understanding, empathetic online friends. My “real life” friends have all abandoned me. No reasons given. Embarrassed?! Tired of my constant cancelling?! Unable to handle my pain?! Whatever the reason, they’re gone. My best friend, secret keeper, confidante, “let’s grow old together” friend, gone. Without a word. It’s easier online. They can’t see my tears, my fears, my hurt, my pain. We talk about it, but it’s not the same as face to face. I see a psychologist. She helps me put things into perspective. My losses, my grief, my fears, my hopes. And yes, I do still have hope. I have to hold on to something. Have a purpose. A reason to wake up and face each new day. Praying for relief, a cure, strength, positive thoughts. Helping others going through similar circumstances. It helps me to help them. To feel like I make a difference to someone in physical and emotional pain. To someone depressed, anxious, panic-filled, like me. We’re strong for each other. Hold each other up. Always reachable. Through new meds, side effects, tests, diagnoses. Bringing laughter to a dark time. But always praying for better days ahead. We must. There is no alternative. Not for me. #AlwaysKeepFighting
The basics of CBT By Tammy Rome
There is a growing body of research to support the use of Cognitive Behavioral Therapy as part of an integrative approach to migrainetreatment. CBT won’t replace headache specialists, preventive therapies, or acute medical interventions. It can help with one of our biggest triggers though.
Stress
Many migraineurs cite stress as their #1 trigger. The theory is that CBT can help patients increase their tolerance level and reduce the number of attacks triggered by stress. One of the strategies used in CBT is to challenge and change the way a patient thinks aboutmigraine as it relates to their lives.
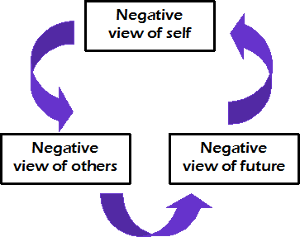
Negative feedback loop
It starts with the idea that negative thinking patterns about yourself, others, and your future create a self-sustaining feedback loop that can affect your whole outlook on life. Breaking the cycle of negative thinking requires us to change the way we think about ourselves, our relationship to others, and our outlook on the future. The way with think about migraine can become an ever-increasingly negative pattern. We can break that cycle by catching our thinking mistakesand correcting those errors.

It works for me
I am just as guilty as everyone else of getting caught in this negative thought/belief pattern many times. Because I have comorbid depression, I am more susceptible to giving in to this kind of thinking. I have to work harder to make sure my thoughts are consistent with reality. The use of CBT strategies has helped to keep my depressive symptoms in remission. It also helps me to manage stress better so I am less vulnerable to those nasty let-down migraine attacks.
Thinking errors
#1 – Drawing a broad conclusion based on irrelevant or insufficient evidence.
Example: “This is my last option.”
I made this mistake when I pursued a “cure” by trying to qualify fortrigger site release surgery. I believed it was the only availabletreatment in my city. That wasn’t true. I just wasn’t willing to look hard enough. I was in a hurry to find a solution, so I didn’t do all of my homework. If you’d asked me back then, I would have denied it. However, the fact that I found several other options after I’d been turned down for surgery proves that my thinking was faulty.
#2 – Focusing on a single aspect of a situation and ignoring others
Example: “There’s nothing left to try.”
I made this mistake when I found out I didn’t qualify for trigger site release surgery. Because I focused on surgery as my only option, I was devastated when it didn’t work out. It took me weeks to finally recognize the truth. There were other treatments to try and otherdoctors to see. I just had to look harder. I tried two more doctors and 6 more treatments before finally finding my current doctors and effective treatments.
#3 – Exaggerating the importance of undesirable events
Example: “I can’t take one more day.”
This was my thinking after getting turned down for surgery. That thought nearly drove me to take my own life. It seems silly now, but in the middle of those thoughts I couldn’t break free. I was so tired of hurting all the time. At least for me, surgery was a passive way to have somebody else fix my problem. In truth, I could tolerate many more days. I know this now because I have done it. If someone had told me in the middle of that darkness that I would face at least 2 more years before getting results, I probably would have given up. Thankfully I was able to focus on getting through one day at a time. Gradually I was able to cope for several days, looking forward to that next appointment. Before long, I had abandoned my lethal plans. My outlook changed because I was able to change how I saw myself and my doctors.
#4 – Underplaying the significance of an event
Example: “I’m fine.”
Don’t we all say this? We minimized our own pain because we rationalize that 1) no one cares to know the truth, 2) we’ve been worse off, or 3) we really don’t want the negative attention. By doing this, we downplay the severity of our symptoms. What’s worse, we do it with our doctors! I’m not suggesting we exaggerate our experiences. Let’s just be honest – any single migraine attack sucks. We’re not fine. We may be fine in a few hours or days, but in the middle of an attack, we are anything but fine.
#5 – Drawing a broad negative conclusion based on a single insignificant event
Example: “Doctors are no help.”
We make a sweeping generalization about all doctors without having tried to work with more than a handful. To be honest, there are some doctors who aren’t any help to us. But that doesn’t mean none of them can help. I know this because I work with two amazing doctors who have helped me a great deal. Neither one of them are UCNS certified and you won’t find them listed on any registry. I’ve also met some very caring, helpful headache doctors. They’re not my doctors, but I know they are helpful because my friends are helped by them. Many of us make this mistake when our doctor tells us there are no more options to try. Just because one, or two, or ten doctors run out of options doesn’t mean there aren’t doctors with new ideas who can help us.
#6 – Attributing the negative feelings of others to yourself
Example: “My husband blames me for always being in pain.”
I made this thinking error many times. When I finally started inviting my husband to talk about the effects of migraine on his life, I learned something very different. Sure, he was frustrated, angry, resentful, and exhausted. He didn’t blame me. He blamed migraine. There’s a big distinction. I get frustrated, angry, resentful, and exhausted because of migraine, too. Once we both realized we were angry about the same thing, we were able to view each other as partners again. The antidote to this mistake is to talk with the person. Ask questions. Listen carefully. Keep an open mind. It may feel as though you are the target of someone’s negative emotions, but that doesn’t make it true. Even if someone does blame you for your migraine, that isn’t necessarily true. They may be guilty of thinking mistakes too.
Interested in learning more about Cognitive Behavioral Therapy and how it can help you with migraine? More articles are in the works that will address different CBT strategies you can use at home.
If you are not familiar with CBT, it might also be a good idea to find a therapist who specializes in CBT for chronic pain. A good starting place is the “Find a Healthcare Provider” tool at ACHEnet.org. When you search, make sure to select the Psychiatry/Psychology/Behavioral Medicine option under Specialty. The providers listed are those who have a good understanding of the impact that migraine has on a patient’s life. They will likely be more sympathetic to your challenges than the average CBT therapist.
Have Fibromyalgia and Migraines?
 Study Shows an Increased Risk of Suicide
Study Shows an Increased Risk of Suicide

A new study published in the journal Neurology says that people who suffer from fibromyalgia and migraines are at increased risk of suicide.
Researchers from the University of Taipei surveyed 1,318 people with migraine headaches, and 10.1% of them also had fibromyalgia. Four out of five of the survey respondents were women.
The results didn’t surprise Dr. Ginevra Liptan, who founded the first practicedevoted to fibromyalgia in Lake Oswego, Oregon.
“Several different studies have demonstrated that that the risk of suicide is higher in fibromyalgia,” she said. ” I think a huge contributor is that people suffering from this ” invisible” illness often feel misunderstood by the medical community- and even sometimes by their family. ”
Of 1,318 patients with migraine included in the analysis 10,1% were found to have co morbid Fibromyalgia. Patients with migraine and co morbid FM had higher headache frequency and headache-related disability, poor sleep quality, and were more depressed/anxious in comparison to those patients who only had migraine.
Of the patients with migraine 27.3% reported suicidal ideation and 6.9% reported suicide attempts. These results were even higher in patients with co morbid FM (58.3% thought about it and 17.6% attempted.).
The researchers also found an association between FM co morbidity and a higher suicide risk in three different migraine subgroups, i.e., migraine without aura, migraine with aura, and chronic migraine. Importantly, FM co morbidity was found to be a predictor of suicidal ideation and attempts in patients with migraine.
Based on these results the authors believe that co morbid FM is associated with a high risk of suicide in migraine patients and awareness of suicide risk should be increased in this specific group of people.
Chronic pain sufferers of all indications are at increased risk of suicide. National Pain Report reported on how NASCAR legend, Dick Trickle, ended his life because of chronic back pain.
If you do not already have a mental health professional as part of your pain management team, you should consider it.
If you or a loved one are in emotional distress or have suicidal thoughts, the National Suicide Prevention Lifeline has counselors available 24 hours day, seven days a week, at 800-273-TALK (8255).
Medication Overuse Headache by Migraine Pal
One of the biggest stumbling blocks for migraineurs, particularly those who have had migraines for years, is medication overuse headaches (MOH).
MOH is the official classification for the common term “rebound headaches”. These are headaches (and even migraines) which occur because of the medication and drugs we’re taking. Typically it occurs when taking medication too often which causes a physical dependence on the drug. When the medication is stopped withdrawal symptoms are experienced and result in a headache or migraine.
MOH often goes unnoticed. Many doctors fail to ask about the frequency and type of medication you’re taking and if there not looking for it, it’s easily missed.
If you experience daily migraine attacks or headaches, there is a 30% to 50% chance you overuse acute medications.
Up to 80% of those who visit migraine headache specialty clinics either overuse acute medication or already have MOH.
MOH is a complication of migraine. It is a secondary condition as a result of the overuse of treatment for the primary migraine or headache. Even if an individual has migraines, MOH becomes the prioritised condition to treat before any progress can be made on the underlying migraine condition. This is the case even if migraines caused MOH in the first place.
MOH is extremely important to address first and foremost. MOH can block or reduce the effectiveness of other treatments. It can be extremely difficult to reduce your migraine frequency whilst you have MOH.
For most migraineurs, they don’t even realise they have MOH. For others, they might feel trapped and concerned about withdrawal symptoms. As you’ll discover from this guide, MOH is very treatable with strong success rates. By addressing MOH, you can get back to improving your migraine condition.
Read the complete MOH guide at MigrainePal
at MigrainePal
Kind regards,
Carl from MigrainePal
A note from LollipopsAndCandyCanes : If you don’t already follow @migrainepal, you should start. Great articles, advice, recommendations, and empathy.
Headache Help: Q&A with Hossein Ansari, MD
Headaches are the most common pain issue brought to physicians and a major reason cited for missed work and school days. Although most headaches are benign, some headaches are disabling enough to compromise a person’s ability to work, socialize and exercise. The financial burden of headaches on the afflicted is currently believed to be greater than that of diabetes, asthma or high blood pressure.
Migraines are also now viewed as a progressive disease which, like heart disease or high blood pressure, may worsen and become more difficult to treat over time. Hossein Ansari, MD, a board-certified neurologist who specializes in diagnosing and treating headaches and facial pain, talks about how to differentiate a migraine from an ordinary headache and potential treatments.
Question: What is a migraine?
Answer: A migraine is a complex neurologic disease with a genetic basis and is not synonymous with a severe headache. Migraine suffers may experience symptoms we call aura without ever having headaches. Aura symptoms can be visual (e.g., seeing dots and lines) or sensory (e.g., numbness on the cheeks, arms or legs) or speech-related.
Q: What are some symptoms suggesting that I should seek medical help for my headaches?
A: Individuals should seek immediate referral to a neurologist, preferably a headache specialist, if they experience any of the following: a stiff neck or fever with a headache or a headache that gets worse when lying down; constant numbness, dizziness, weakness or difficulty with speech; confusion, drowsiness or loss of consciousness with headaches; headaches for the first time after age 50 or “the worst headache of your life.” Those who develop headaches while on an immunosuppressant, such as chemotherapy or steroids, should also seek immediate help from a neurologist.
Q: What is known about the relationship between foods and fasting in triggering migraines? What about alcoholic beverages?
A: Artificial sweeteners, nitrates (often found in processed meats) and MSG can induce migraines. Most migraine triggers assumed to be food-related, though, are actually part of the migraine itself. By this I mean that before a headache begins, a person may experience food cravings or aversions. Fasting and alcohol, particularly red wine, can also trigger migraines.
Q: What can I do to prevent migraines?
A: We recommend regular, light exercise at least three days a week. Yoga, tai-chi and other mind-body practices are particularly beneficial. Multiple studies show that migraines often become chronic among overweight individuals. For this reason, attaining or maintaining a healthy, normal weight is critical. Drinking plenty of fluids, avoiding stress and getting adequate sleep are also important.
Q: How do you differentiate a sinus headache from a migraine?
A: Headache specialists consider the term sinus headache a misnomer. Most persons who think they have sinus headaches actually suffer from migraines.
Q: What about hormone fluctuations and migraines?
A: Hormonal fluctuations associated with the menstrual cycle can bring on migraines. Hormone therapies that regulate estrogen levels can avert attacks. Women who have migraines with aura should avoid certain birth control pills to prevent an increased risk of stroke.
Q: What are the most promising investigational treatments in the pipeline?
A: The most promising interventional treatment is a surgical procedure known as a migraine trigger point deactivation surgery. There is also a new drug on the horizon – a calcitonin gene-related peptide (CGRP), long postulated to play a key role in the pathophysiology of migraines – that has shown promise in preclinical and clinical trials.
Source: UC San Deigo Health Headache Help: Q&A with Hossein Ansari, MD
Another Dawn, Another Day
Here I am again. 3:30 am. Typing about my feelings. Wanting so badly to be asleep. Deep, restorative sleep. No dreams sleep. Reassuring sleep. Rejuvenating sleep. But sleep is becoming a dream in itself. Short, light sleep is what I get. If I go too deep into REM, the nightmares come. I don’t remember them as a whole. Just bits and pieces. They’re dark, scary, fraught with anxiety and panic. Clawing at the light. Begging to wake up. And I do. And it all starts again. A cycle of pain, fear, sleep, wake, dream, flashes of memory, dark, light. Too afraid to fall asleep, too exhausted not to. Endless circles of day and night blending together. Dawn is my time to think, type, try to put down into words what is happening to me. Not to scare others, not to scare myself. But to seek out those who feel as I do. For reassurance. For comfort. For ideas. Suggestions. To know I’m not alone. Because at 3:00 am, I feel alone. #AlwaysKeepFighting 
The Search For Meds
PAIN MANAGEMENT 08.06.2015
Pain Patients Say They Can’t Get Meds After Illegal Rx Drug Crackdown
Pharmacies’ allocations are being restricted by wholesalers
by Rachel Gotbaum
Kaiser Health News
The accident happened 10 years ago when Chris Young was 35. He owned a salvage yard in Maui, Hawaii, and his employee had hoisted a junker on a machine called an excavator when the hydraulics gave out. The car fell on him from above his head, smashing his spine.
“He was crushed accordion-style,” says his wife Lesley.
The accident left Young with a condition known as “partial paraplegia.” He can’t walk and he needs a wheelchair, but he does have some sensation in his legs. Unfortunately for Young, that sensation is often excruciating pain.
“It feels like electric shocks, like lightning bolts going down my legs. And when it gets down to the bottom, it feels like someone is driving a big metal spike up my legs,” says Young.
To control the pain, Young, who has since moved to Florida, needs high doses of narcotic painkillers, but he can’t always fill his doctor’s prescription. He is not alone. In what may be an unintended side effect of a crackdown on prescription drug abuse, Young and other legitimate chronic pain patients are having increasing trouble getting the medicine that allows them to function on a daily basis.
Young’s pharmacy runs out every month.
“They just do not have the medications because they have run out of their allocation within the first week,” he says. “It’s just that bad, where I know I am going to end up in the E.R. because of not having my medications. We don’t know what to do. We’ve tried everything.”
Young’s pharmacist is Bill Napier, who owns the small, independent Panama Pharmacy in Jacksonville. Napier says he can’t serve customers who legitimately need painkillers because the wholesalers who supply his store will no longer distribute the amount of medications he needs.
“I turn away sometimes 20 people a day,” says Napier.
Last year Napier says federal Drug Enforcement Administration agents visited him to discuss the narcotics he dispensed.
“They showed me a number, and they said that if I wasn’t closer to the state average, they would come back. So I got pretty close to the state average,” Napier says. He says he made the adjustment “based on no science, but knowing where the number needed to be. We had to dismiss some patients in order to get to that number.”
According to Napier, DEA agents took all of his opioid prescriptions and held on to them for seven months. Napier hired a lawyer and paid for criminal background checks on his patients taking narcotics to help him decide which ones to drop.
“We’re being asked to act as quasi-law enforcement people to ration medications,” says Napier. “I have not had training in the rationing of medications.”
Until a few years ago, Florida was considered the epicenter for the trafficking of illegal prescription narcotics. The DEA and local law enforcement shut down more than 250 so-called “pill mills” — clinics where doctors could sell narcotics directly to people for cash. Now Florida doctors can no longer dispense narcotics directly to patients. Wholesalers, who paid to settle claims for failing to report suspicious orders of drugs, now limit the amount they sell to pharmacies, Napier says.
Jack Riley, who is acting deputy administrator of the DEA, credits a decline in opioid overdose deaths in Florida with an upsurge in law enforcement activity. The problem of addiction and the drug trade is dire, he says.
“A hundred and twenty people a day die of drug abuse in this country,” Riley said. “If that doesn’t get your attention, I don’t think anything can.”
Riley also says law enforcement efforts cannot be blamed for any claim of rationing of painkillers.
“I’m not a doctor. We do not practice medicine. We’re not pharmacists. We obviously don’t get involved in that,” said Riley. “What we do do is make sure the people that have the licenses are as educated as possible as to what we’re seeing, and that they can make informed decisions as they do dispense.”
Doctors, too, say DEA enforcement actions have made it harder for them to prescribe narcotics. Last year, hydrocodone products, such as Vicodin, were changed to Schedule II status, meaning they have a high potential for abuse and cannot be prescribed in large quantities.
“What we’ve seen is dramatic reductions in our ability to provide appropriate care for our patients in pain,” says Dr. R. Sean Morrison, director of the palliative care program at Mount Sinai Hospital in New York.
Morrison’s patient Ora Chaikin has been taking high levels of narcotics for years to control her pain. She has had multiple surgeries because her bones and ligaments disintegrate, a problem caused by rheumatoid arthritis and other autoimmune diseases. But Chaikin, who lives in Riverdale, N.Y., says her mail order pharmacy, CVS/caremark, has been denying her medications.
“Every month there’s a reason they won’t give me my medication,” says Chaikin. “Sometimes it’s ‘Well, why are you taking this dose?’ ‘My doctor prescribed it.’ ‘Well, why did your doctor prescribe so much?’ ‘Ask my doctor,'” she recounts. “That’s the dose that works for me and you’re made to feel like a drug addict.”
The DEA investigated both CVS and Walgreens, and both pharmacy chains settled civil suits in 2013 for record-keeping violations of the Controlled Substances Act. Walgreens paid an $80 million civil penalty, and CVS paid an $11 million penalty.
Riley, of the DEA, says it would be wrong to draw a line between these actions and problems like those Chaikin is experiencing. “If there is a chilling effect, it’s clearly not at our direction,” Riley said. “We’re simply enforcing the law, taking bad people off the street and really trying to interrupt the supply of illegal prescriptions.”
In a statement, CVS/caremark said that the dosage of pain medication prescribed to Chaikin “exceeded the recommended manufacturer dosing.” It also said that she “continued to receive her controlled substance prescriptions from CVS/caremark without interruption.”
CVS/caremark said it has a legal obligation to make sure controlled substance prescriptions are for legitimate ailments and “that patients are receiving safe medication therapy, including appropriate dosing.”
Ora Chaikin’s wife, Roseanne Leipzig, who is a geriatrician and palliative care physician, says when it comes to narcotics, there is nothing in medical literature that says a dose is too high.
“There is no maximum dose for narcotics,” she says. “It’s the dose you need to take care of the pain.”
The Florida Board of Pharmacy, which is responsible for licensing pharmacists and educating them on safe practice, has heard enough complaints from pain patients that it is addressing the issue in public meetings. In June, Lesley Young testified before the board on behalf of her husband. She said she has driven more than 100 miles trying to find a pharmacy that would fill her husband’s prescriptions for painkillers.
“I’ve had to do the pharmacy crawl like many of us here,” Lesley told the board. “I’ve been the one who had to go in and beg, crying, with stacks of his medical records, with stacks of imaging, only to get turned away, often rudely, saying ‘We don’t deal with those kinds of patients.'”
The next Florida Board of Pharmacy hearing is set for Monday. A representative of the DEA has been invited to attend.
This story was produced in a collaboration between NPR’s Here & Now and Kaiser Health News.
This article, which first appeared Aug. 5, 2015, also ran on NPR’s Here and Now. It was reprinted from kaiserhealthnews.org with permission from the Henry J. Kaiser Family Foundation. Kaiser Health News, an editorially independent news service, is a program of the Kaiser Family Foundation, a nonprofit, nonpartisan health policy research and communication organization not affiliated with Kaiser Permanente.
LAST UPDATED 08.06.2015
